Autores: Eduardo Botello / Tomás Zamora
Introduction: Hip fracture patients have been severely affected by the COVID-19 pandemic; however, the sub acute effects of a concomitant SARS-CoV-2 infection and the outcomes in highly exposed developing countries are still unknown. Our objective is to describe the morbidity and mortality of elderly patients admitted for a hip fracture during the COVID-19 pandemic in Chile, with a minimum 90-day follow-up. Also, to elucidate predictors for mortality and to compare mortality results with the pre-pandemic era. Material and methods: Multicentric retrospective review of patients admitted for a fragility hip fracture in 3 hospitals during the COVID-19 pandemic, and during the same time in 2019. All clinical information and images were recorded, and patients were followed for a minimum of 90-days. Morbidity and mortality were the primary outcomes. Uni/multivariable models were performed to elucidate predictors for mortality utilizing the Weibull’s regression. Results: Three hundred ninety-one cases were included. From the 2020 cohort (162 patients), 24 (15%) had a concomitant SARS-CoV-2 infection. Fourteen patients (58%) tested positive after admission. The COVID-19(+) group had a higher risk of in-hospital, 30-day, and 90-day mortality (p < 0.001). They also had a prolonged hospital stay and presented with more complications and readmissions (p < 0.05). Only COVID-19(+) status and older age were independent predictors for mortality with a HR = 6.5 (p = < 0.001) and 1.09 (p = 0.001), respectively. The 2020 cohort had twice the risk of mortality with a HR = 2.04 (p = 0.002) compared to the 2019 cohort. However, comparing only the COVID-19 (-) patients, there was no difference in mortality risk, with a HR = 1.30 (p = 0.343). Discussion: The COVID-19 pandemic has significantly affected healthcare systems and elderly patients. Conclusions: Hip fracture patients with a concomitant SARS-CoV-2 virus infection were associated with increased morbidity and mortality throughout the first 3 months. COVID-19 status and older age were significant predictors for mortality. Efforts should be directed into nosocomial infection reduction and prompt surgical management. Level of evidence: Level III.
DOI:10.1007/978-3-030-95738-4_4
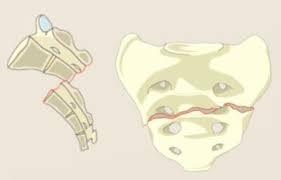
Autores: Arturo Meissner-Haecker / Claudio Diaz-Ledezma / Ianiv Klaber / Tomas Zamora
Background Sacral fractures treatment frequently involves both spine and pelvic trauma surgeons; therefore, a consistent communication among surgical specialists is required. We independently assessed the new AOSpine sacral fracture classification’s agreement from the perspective of spine and pelvic trauma surgeons. Methods Complete computerized tomography (CT) scans of 80 patients with sacral fractures were selected and classified using the new AOSpine sacral classification system by six spine surgeons and three pelvic trauma surgeons. After four weeks, the 80 cases were presented and reassessed by the same raters in a new random sequence. The Kappa coefficient (κ) was used to measure the inter-and intra-observer agreement. Results The inter-observer agreement considering the fracture severity types (A, B, or C) was substantial for spine surgeons (κ= 0.68 [0.63 – 0.72]) and pelvic trauma surgeons (κ= 0.74 (0.64 – 0.84). Regarding the subtypes, both groups achieved moderate agreement with κ= 0.52 (0.49 – 0.54) for spine surgeons and κ= 0.51 (0.45 – 0.57) for pelvic trauma surgeons. The intra-observer agreement considering the fracture types was substantial for spine surgeons (κ= 0.74 [0.63 – 0.75]) and almost perfect for pelvic trauma surgeons (κ= 0.84 [0.74 – 0.93]). Concerning the subtypes, both groups achieved substantial agreement with, κ= 0.61 (0.56 – 0.67) for spine surgeons and κ= 0.68 (0.62 – 0.74) for pelvic trauma surgeons. Conclusion This classification allows an adequate communication for spine surgeons and pelvic trauma surgeons at the fracture severity type, but the agreement is only moderate at the subtype level. Future prospective studies are required to evaluate whether this classification allows for treatment recommendations and establishing prognosis in patients with sacral fractures.

Autores: Dr. Tomás Zamora
Benign cartilaginous neoplasms are among the most common bone lesions. Enchondromas are the classical presentation of them and are usually found incidentally. Their clinical presentation can range from an asymptomatic lesion in an adult to multiple lesions as part of a syndrome in a younger patient. If the clinical and radiological presentation is characteristic, enchondromas can be treated non-operatively with observation alone. However, in certain circumstances, the differential diagnosis among a benign enchondroma or an atypical cartilaginous neoplasm/low-grade chondrosarcoma can be difficult and might need further investigations and a multidisciplinary approach. In cases of symptomatic lesions, diagnostic uncertainty, or a pathological fracture, curettage and grafting with or without osteosynthesis is usually the treatment of choice.

Autores: Tomas Zamora / Felipe Sebastian Sandoval / Hugo Demandes / Javier Serrano
Introduction: Hip fracture patients have been severely affected by the COVID-19 pandemic; however, the sub acute effects of a concomitant SARS-CoV-2 infection and the outcomes in highly exposed developing countries are still unknown. Our objective is to describe the morbidity and mortality of elderly patients admitted for a hip fracture during the COVID-19 pandemic in Chile, with a minimum 90-day follow-up. Also, to elucidate predictors for mortality and to compare mortality results with the pre-pandemic era. Material and methods: Multicentric retrospective review of patients admitted for a fragility hip fracture in 3 hospitals during the COVID-19 pandemic, and during the same time in 2019. All clinical information and images were recorded, and patients were followed for a minimum of 90-days. Morbidity and mortality were the primary outcomes. Uni/multivariable models were performed to elucidate predictors for mortality utilizing the Weibull’s regression. Results: Three hundred ninety-one cases were included. From the 2020 cohort (162 patients), 24 (15%) had a concomitant SARS-CoV-2 infection. Fourteen patients (58%) tested positive after admission. The COVID-19(+) group had a higher risk of in-hospital, 30-day, and 90-day mortality (p < 0.001). They also had a prolonged hospital stay and presented with more complications and readmissions (p < 0.05). Only COVID-19(+) status and older age were independent predictors for mortality with a HR = 6.5 (p = < 0.001) and 1.09 (p = 0.001), respectively. The 2020 cohort had twice the risk of mortality with a HR = 2.04 (p = 0.002) compared to the 2019 cohort. However, comparing only the COVID-19 (-) patients, there was no difference in mortality risk, with a HR = 1.30 (p = 0.343). Discussion: The COVID-19 pandemic has significantly affected healthcare systems and elderly patients. Conclusions: Hip fracture patients with a concomitant SARS-CoV-2 virus infection were associated with increased morbidity and mortality throughout the first 3 months. COVID-19 status and older age were significant predictors for mortality. Efforts should be directed into nosocomial infection reduction and prompt surgical management. Level of evidence: Level III.
Doi: 10.1177/21514593211024509
Autores: Alexander Nedopil / Tomas Zamora / Connor Delman / Stephen Miller Howell
Calipered kinematically aligned (KA) total knee arthroplasty (TKA) restores the patient’s prearthritic joint lines and sets internal-external rotation of the tibial component parallel to the flexion-extension (FE) plane, which is not a mechanical alignment (MA) target. Two asymmetric tibial components designed for MA set the tibial component to either a femoral component (FC) target or a tibial tubercle (TT) target. The study determined the optimal asymmetric tibial component to use with KA as the one with smaller IE deviation from the MA target, greater coverage of tibial resection, and lower incidence of cortical overhang. The study included 40 patients treated with bilateral calipered KA TKA with different asymmetric tibial components in opposite knees. A best-fit of a kinematic tibial template to the tibial resection set the template’s slot parallel to the knee’s FE plane. Each asymmetric tibial component’s anterior-posterior (AP) axis was set parallel to the slot. Computer tomography analysis determined the IE deviation (-internal/+ external) of each tibial component from its MA target, tibial resection coverage by the baseplate and insert, and incidence of cortical overhang. The patient-reported Forgotten Joint Score (FJS) and Oxford Knee Score (OKS) determined outcomes. The mean IE deviation from the MA target was 2 degrees external for the FC-target asymmetric tibial component and -8 degrees internal for the TT-target asymmetric tibial component (p < 0.001). Tibial resection coverage by the baseplate (insert) was 88% (84%) for the FC target and 84% (79%) for the TT target (p < 0.001 for baseplate and insert). The FC target insert covered 3 mm more of the posterolateral resection (p < 0.001). Posteromedial coverage was comparable. The incidence of cortical overhang was 2.5% for each baseplate. There was no difference in FJS and OKS. When performing calipered KA, the more optimal design was the asymmetric tibial component with the FC target because of the smaller deviation from its MA target and the greater coverage of the tibial resection by the baseplate and insert.
Doi: 10.1055/s-0041-1728815
Autores: Francisco Bengoa / Gerardo Vicencio / Daniel Schweitzer / María Jesús Lira / Tomas Zamora / Ianiv Klaber
Purpose Deep vein thrombosis (DVT) is a common complication in hip fracture patients, associated with significant morbidity and mortality. Research has focused on postoperative DVT, with scant reports on preoperative prevalence. The aim of this study was to describe the prevalence of preoperative DVT in patients accessing medical care ≥ 48 h after a hip fracture. Methods We included elderly patients admitted ≥ 48 h after sustaining a hip fracture, between September 2015 and October 2017. Patients with a previous episode of DVT, undergoing anticoagulation therapy, with pathologic fractures or undergoing cancer treatment were excluded. Of 273 patients, 59 were admitted at least 48 h after the fracture. DVT screening by Doppler ultrasound of both lower extremities was carried upon hospital admission. We recorded age, sex, Charlson comorbidity index and ASA score, fracture type, time since injury, time from admission to surgery and total length of hospital stay. Results We studied 41 patients, 79 (± 10.34) years old. The delay from injury to admission was 120 h (48–696 h). Seven patients (17.1%) had a DVT upon admission. There were no significant differences between patients with and without DVT, regarding time from admission to surgery or the total length of the hospital stay. Conclusions The prevalence of DVT in patients admitted ≥ 48 h after a hip fracture was 17.1%. The diagnosis and management of DVT did not increase time to surgery or hospital stay. Our results suggest routine screening for DVT in patients consulting emergency services ≥ 48 h after injury.
DOI:10.1007/s00068-018-1059-8
Autores: Dr. Tomas Zamora / Dr. Donald S Garbuz / Dr. Nelson Greidanus / Dr. Bassam A Masri
Aims: Our objective is to describe our early and mid-term results with the use of a new simple primary knee prosthesis as an articulating spacer in planned two-stage management for infected knee arthroplasty. As a second objective, we compared outcomes between the group with a retained first stage and those with a complete two-stage revision. Methods: We included 47 patients (48 knees) with positive criteria for infection, with a minimum two-year follow-up, in which a two-stage approach with an articulating spacer with new implants was used. Patients with infection control, and a stable and functional knee were allowed to retain the initial first-stage components. Outcomes recorded included: infection control rate, reoperations, final range of motion (ROM), and quality of life assessment (QoL) including Western Ontario and McMaster Universities osteoarthritis index, Knee Injury and Osteoarthritis Outcome Score, Oxford Knee Score, 12-Item Short-Form Health Survey questionnaire, and University of California Los Angeles (UCLA) activity score and satisfaction score. These outcomes were evaluated and compared to additional cohorts of patients with retained first-stage interventions and those with a complete two-stage revision. Mean follow-up was 3.7 years (2.0 to 6.5). Results: Eight knees failed directly related to lack of infection control (16%), and two patients (two knees) died within the first year for causes not directly related, giving an initial success rate of 79% (38/48). Secondary success rate after a subsequent procedure was 91% (44/48 knees). From the initially retained spacers, four knees (22%) required a second-stage revision for continuous symptoms and one (5%) for an acute infection. There were no significant differences regarding the failure rate due to infection, ROM, and QoL assessment between patients with a retained first-stage procedure and those who underwent a second-stage operation. Conclusion: Our protocol of two-stage exchange for infected knee arthroplasties with an articulating spacer and using new primary knee implants achieves adequate infection control. Retained first-stage operations achieve comparable results in selected cases, with no difference in infection control, ROM, and QoL assessment in comparison to patients with completed two-stage revision surgery
DOI:10.1302/0301-620X.102B7.BJJ-2019-1443.R1
Autores: Dr. Ianiv Klaber /Dr. Pablo Besa /Dr. Felipe Sebastian Sandoval /Dr. Daniel Lobos /Dr.
Tomas Zamora /Dr. Daniel Schweitzer /Dr. Julio Urrutia
Background : A new AO classification for intertrochanteric fractures was recently published; no studies have evaluated its inter- and intra-observer agreement. Methods : Six evaluators (three hip subspecialists and three residents) assessed radiographs of 68 intertrochanteric fractures; fractures were classified using the original and the new AO classifications. The cases were displayed in a random sequence after a six-week interval for repeat evaluation. We used the Kappa coefficient (k) to determine inter- and intra-observer agreement. Results : Inter-observer agreement was slight (k= 0.128 [0.092-0.170]) using the original and fair (k= 0.250 [0.186-0.327]), with the new AO classification. Orthopedic residents exhibited better agreement than hip surgeons using the original classification (k= 0.302 [0.210-0.416] and k= -0.018 [-0.058-0.029], respectively) and the new classification (k= 0.388 [0.294-0.514] and k= 0.109 [0.031-0.192], respectively). Using both classifications as dichotomous variables (stable or unstable patterns), the agreement was slight (k= 0.158 [0.074-0.246]) using the original classification and moderate (k= 0.425 [0.308-0.550]) with the new AO classification. Intra-observer : The agreement was fair using the original (k= 0.350 [0.278-0.424]) and the new (k= 0.295 [0.239 to 0.353]) AO classifications, respectively. Residents had better agreement than hip specialists using the original (k= 0.405 [0.303-0.512]) versus (k= 0.292 [0.193-0.293]) and the new classification (k= 0.449 [0.370 to 0.528] versus k= 0.129 [0.064 to 0.208]). Conclusion : The inter-observer agreement using the new AO classification was significantly better than using its original version. Also, the new AO classification system allowed better agreement when distinguishing stable from unstable patterns.
DOI:10.1016/j.injury.2020.07.020
Autores: Dr. Alexander Nedopil /Dr. Tomas Zamora /Dr. Trevor Shelton /Dr. Stephen Miller Howell /Dr. Maury L. Hull
Background : A new AO classification for intertrochanteric fractures was recently published; no studies have evaluated its inter- and intra-observer agreement. Methods : Six evaluators (three hip subspecialists and three residents) assessed radiographs of 68 intertrochanteric fractures; fractures were classified using the original and the new AO classifications. The cases were displayed in a random sequence after a six-week interval for repeat evaluation. We used the Kappa coefficient (k) to determine inter- and intra-observer agreement. Results : Inter-observer agreement was slight (k= 0.128 [0.092-0.170]) using the original and fair (k= 0.250 [0.186-0.327]), with the new AO classification. Orthopedic residents exhibited better agreement than hip surgeons using the original classification (k= 0.302 [0.210-0.416] and k= -0.018 [-0.058-0.029], respectively) and the new classification (k= 0.388 [0.294-0.514] and k= 0.109 [0.031-0.192], respectively). Using both classifications as dichotomous variables (stable or unstable patterns), the agreement was slight (k= 0.158 [0.074-0.246]) using the original classification and moderate (k= 0.425 [0.308-0.550]) with the new AO classification. Intra-observer : The agreement was fair using the original (k= 0.350 [0.278-0.424]) and the new (k= 0.295 [0.239 to 0.353]) AO classifications, respectively. Residents had better agreement than hip specialists using the original (k= 0.405 [0.303-0.512]) versus (k= 0.292 [0.193-0.293]) and the new classification (k= 0.449 [0.370 to 0.528] versus k= 0.129 [0.064 to 0.208]). Conclusion : The inter-observer agreement using the new AO classification was significantly better than using its original version. Also, the new AO classification system allowed better agreement when distinguishing stable from unstable patterns.
DOI:10.1055/s-0040-1710367
Autores: Dr. Tomas Zamora / Dr. Ianiv Klaber / Dr. Joaquin Ananias / Dr. Francisco Bengoa / Dr. Eduardo Botello / Dr. Pedro Pablo Amenábar / Dr. Daniel Schweitzer
Background : A new AO classification for intertrochanteric fractures was recently published; no studies have evaluated its inter- and intra-observer agreement. Methods : Six evaluators (three hip subspecialists and three residents) assessed radiographs of 68 intertrochanteric fractures; fractures were classified using the original and the new AO classifications. The cases were displayed in a random sequence after a six-week interval for repeat evaluation. We used the Kappa coefficient (k) to determine inter- and intra-observer agreement. Results : Inter-observer agreement was slight (k= 0.128 [0.092-0.170]) using the original and fair (k= 0.250 [0.186-0.327]), with the new AO classification. Orthopedic residents exhibited better agreement than hip surgeons using the original classification (k= 0.302 [0.210-0.416] and k= -0.018 [-0.058-0.029], respectively) and the new classification (k= 0.388 [0.294-0.514] and k= 0.109 [0.031-0.192], respectively). Using both classifications as dichotomous variables (stable or unstable patterns), the agreement was slight (k= 0.158 [0.074-0.246]) using the original classification and moderate (k= 0.425 [0.308-0.550]) with the new AO classification. Intra-observer : The agreement was fair using the original (k= 0.350 [0.278-0.424]) and the new (k= 0.295 [0.239 to 0.353]) AO classifications, respectively. Residents had better agreement than hip specialists using the original (k= 0.405 [0.303-0.512]) versus (k= 0.292 [0.193-0.293]) and the new classification (k= 0.449 [0.370 to 0.528] versus k= 0.129 [0.064 to 0.208]). Conclusion : The inter-observer agreement using the new AO classification was significantly better than using its original version. Also, the new AO classification system allowed better agreement when distinguishing stable from unstable patterns.
DOI:10.1177/2309499019836160
Autores: Dr. Tomas Zamora.
Resumen La localización del osteocondroma en la tibia distal es poco frecuente y su crecimiento con compromiso y deformidad del peroné distal es aún más raro, haciéndolo una condición más sintomática que en otras ubicaciones. Factores como la severidad de los síntomas, deformidad progresiva del tobillo, complicaciones sindesmóticas, riesgo de fractura patológica o transformación maligna, junto con nuevas y mejores técnicas quirúrgicas, han llevado a que el manejo expectante de esas lesiones sea excepcional y escasamente reportado. Presentamos el caso de un joven de 17 años con osteocondroma solitario interóseo tibio distal sintomático y compromiso fibular, que fue exitosamente manejado en forma expectante. A los 5 años de seguimiento clínico-radiológico no presenta complicaciones y la lesión se mantiene estable.
DOI:10.1055/s-0039-1677832
Autores: Tomas Zamora, Ianiv Klaber, Francisco Bengoa, Eduardo Botello
Background: As the population ages, patients exposed to osteoporotic fractures increase, especially hip fracture, which is the most severe and costly. Aim: To characterize surgical practices in the management of hip fractures in older patients through a nationwide survey of specialized hip surgeons dedicated to the care of these patients. Material and methods: A survey composed of 32 questions was formulated, including demographic factors, preoperative evaluation, definitive treatment, and postoperative management. It was sent to 140 specialists. 84 of them replied (61%), and 71 answers were included. Results: Eighty six percent of respondents agreed that orthogeriatric management is fundamental in the outcome of these patients, but only 73% had the collaboration of an internist or a geriatrician. Although 97% considered 72 hours or less the ideal time to perform surgery, only 52% of the respondents declared performing surgery within that timeframe, with differences between private and public system. Regarding surgical treatment, 94-98% of femoral neck fractures are treated with an arthroplasty and 98-99% of per-subtrochanteric fractures are treated with internal fixation and osteosynthesis. Osteoporosis treatment is only carried out by 51% of the respondents and with significant variation. Conclusions: This survey shows that there is agreement in surgical practice between specialists treating these patients, but clear differences in preoperative optimization, treatment timeframe, and post fracture medical treatment.
10.4067/s0034-98872019000200199